


Let us learn from an example
A 90 years old male presented with left sided abdominal pain and after evaluation was found to have left Kidney mass (Cancer). The family was apprehensive given the age of patient and disease so they came to Fortis hospital Mohali for further treatment and consulted Dr Rohit Dadhwal Consultant Urology, Andrology and Robotic Surgery. After careful assessment he was electively planned for Robotic radical nephrectomy (Removal of Kidney along with tumor) on 22/4/23. Surgery was uneventful with minimal blood loss, patient was kept in ICU for 1 day and was shifted to ward next day. Recovery was smooth and he was discharged 3 days after the surgery. Currently patient is leading a healthy normal life.
Robot-aided surgery is the latest form of minimal invasive surgery and provides a 3D view of the operative field via a special camera inserted into the body of the patient. Parts of the body which are difficult to reach with the human hand can be accessed by robot-assisted arms that can rotate 360 degrees. Patients have minimal blood loss, less pain, less scarring, shorter hospital stay and faster recovery.
A 26 years old young healthy female presented with obstructive lower urinary tract symptoms (LUTS) like weak stream, staining to void, incomplete evacuation. On examination abdomen and external genitalia along with urethra and meatus were normal. Her per vaginal examination revealed large mass anteriorly which was mobile not fixed to surrounding structures. Further MRI pelvis confirmed a mass of size 7×5 cm arising from anterior part of proximal urethra compressing UB neck and hence causing symptoms. On the basis of current findings, a diagnosis of suspected fibroid urethra and bladder neck was made. After explaining all the options, patient was electively planned for Robotic surgery. At this very site i.e. on bladder neck and proximal urethra, there lies the mechanism for voluntary control of urination aka continence mechanism. So the challenge was not only to prevent urethral injury but also prevent leakage of urine. Robotic excision of urethral mass was done electively, after dropping bladder mass could be seen arising from anterior urethra. With the help of fine dissection and good vision we could preserve the vital structures and remove the time which was present so deep in the pelvis. Operative time was around 2 hrs and loss was only 30ml.Patient was made ambulatory on day 1 and was discharged on day 2 of surgery. After more than 2 months of follow-up she is totally continent no stress urinary incontinence. Histopathology has confirmed leiomyoma.
Leiomyoma also known as fibroids are benign tumors arising from smooth muscle cells. They are mostly uterine but they are also seen in gastrointestinal and genitourinary system. Urethral fibroids are extremely rare <45 cases reported and only handful excised via Robotic surgery till now.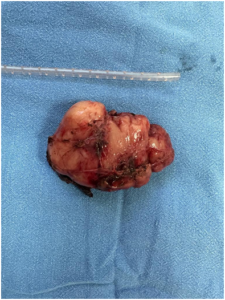
A 72-year-old hypertensive man was undergoing a challenging time due to recurrent urinary tract infections, overflow urinary incontinence, increased frequency and nocturia (condition when one wakes up during the night to urinate). The patient had visited several hospitals in the past and had undergone multiple prostatic surgeries (At least 6) at various hospitals. However, after his condition failed to improve and he presented to our center, Fortis Hospital Mohali, in February this year. After careful examination and focused investigations, he was found to have a giant urinary bladder diverticulum which is an outpouching of normal bladder and an umbilical hernia. The capacity of diverticulum was more than 500 ml and due to failure of it to get emptied during normal urination patient was having high urine retention leading to recurrent infections. By the time he came to the hospital his infection had already become resistant to all antibiotics. To his relief first he was cured of infection and then he was ele tively planned for Robot-assisted Bladder diverticulectomy on 23/2/2023. Robot-assisted surgery is considered as the gold standard treatment in such complicated cases situated in the deep pelvis. The Patient had a smooth post-operative recovery, was able to walk on the next day and was discharged two days after the surgery on 25/2/2023. Per urethral catheter was kept for two weeks and was removed after a cystogram which was normal. Histopathological report showed benign disease and patient is currently leading a normal life. Small Urinary bladder diverticula are not uncommon but giant diverticulum, like in this case is very rare condition and it posed a challenge to treating surgeon. Open, laparoscopic and robotic surgery has been done in the past in the west, but to our knowledge this is the first case done by robotic surgery for giant bladder diverticulum of more than 500ml capacity, anywhere in the world.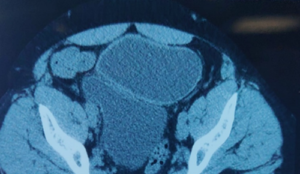
1. CT scan showing normal bladder (arrow head) with giant bladder diverticulum (arrow)
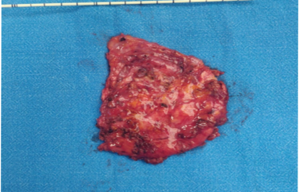
2. Excised diverticular wall
A 39 years old male presented with Obstructive LUTS in the form of weak urinary stream and staining to void along with constipation, for the last 1 year. General examination was unremarkable except for a left undescended testis with poorly developed left scrotum. Ultrasound and CT scan revealed large pelvic mass between rectum and urinary bladder which was causing symptoms. FDG PET showed 16×10 cm mass deep in the pelvis compressing UB neck and rectum with multiple peritoneal and omental metastasis. Tumor marker AFP was 58000 (0-40 ng/ml) indicating high risk of disease. Based on available findings and a biopsy a diagnosis of metastatic NSGCT (Mixed germ cell tumor) Stage IIIC was made. Challenge was first to save life and then to preserve continence, prevent rectum injury along with best tumor control.
Patient first received 3 cycles of chemotherapy (BEP) and when AFP came down to 188 ng/ml and then he was electively planned for surgery. Robotic excision of pelvic mass with excision of peritoneal metastasis with omentectomy was done under GA, total operative time was 6 hrs with blood loss of <100cc. Patient was made ambulatory day 2 and discharged on day 3. He had smooth post operative recovery. HPE report showed necrosis only with no viable tumor. AFP decreased to 38 post surgery and he was further given two more cycles of EP based chemotherapy which was completed in September 23. Currently his AFP is 6 (<7 normal) in June 24 and he is leading a normal life.
Very rare tumor with handful of case reports in literature. Few centers in the world are able to remove it via robotic surgery. Ifdone properly has got excellent results.
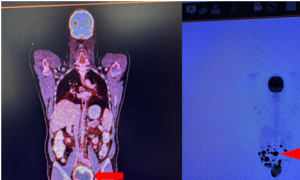
1.PET image showing large tumor (arrow) with multiple omental and peritoneal metastasis (arrow head)
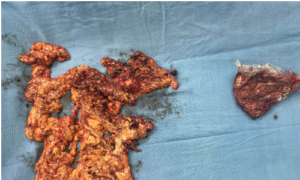
2.Removed omentum and primary tumor

Introduction
It’s fair to say that no one looks forward to surgery, but it may sometimes provide best option for care. One of the many things that makes us humans unique is that we improve with time and continuously try to be better in many aspects. Likewise, evolution of surgical technique can be understood starting from traditional open method then to minimally invasive like laparoscopic technique and now the newest form Robotic surgery.
Why there is need for Robotic surgery?
Traditional open surgery, where a surgeon operates with handheld instruments through a large cut (incision), may be the first method that comes to mind. However, it has got its own complications like large scar, incisional hernia, intestinal adhesions, less precision etc. In view of this less invasiveapproach requiring just a few small cuts, called laparoscopic surgery was developed and for many decades it became standard of care for many surgical conditions. Although laparoscopy decreased many of complications of open surgery there are still limitations with the technique like limited movement of surgical instruments, limited vision, difficulty in suturing and doing complex dissection and suturing. Also if a surgeon has hand tremors, it can cause can serious complications during the procedure. All these necessities led to the invention of Robotic surgery.
It was initially developed for cardiac surgery in 1999. Modern-day Robotic system is, however, predominantly dominated by urological, gynaecological and visceral surgery. In the western world the robotic systems have increasingly become the workhorse in a number of urological units and has replaced laparoscopic modality in many centres. In our beloved country it has gained much of a popularity recently and now is available at major hospitals.
What are the parts of Robotic System?
Da Vinci is most common and most popular robotic system and has got three parts
- SURGEON CONSOLE- Surgeon sits at the console, controlling the instruments while viewing your anatomy in high-definition 3D. With the movements of hand and foot it operates upon the patient remotely.
- PATIENT CART- Positioned alongside the bed, the patient cart holds the camera and instruments that the surgeon controls from the console. Hand and foot movements of console is simulated by the instruments inside the human body
- VISION CART- The vision cart makes communication between components possible and supports the 3D high-definition vision system. It has got an additional screen for the assistant to see.

What all surgeries can be performed by Robotic surgery?
Number of procedures including Colorectal, General surgical, Gynecological, Head and Neck (Trans oral) and Thoracic (related to heart and lungs) can be performed using this but the main field which has got maximum advantage is Urology. Urological procedures have got best cost to benefit ratio as compared to other fields and has revolutionised urological cancer and other disease care in recent decade. Popularly it is used to treat Prostate cancer, Kidney tumors, Urinary bladder and deep pelvic pathologies, large ureteric stones and other benign conditions. Currently it is also used for kidney transplant in selected centres. For tumors it has got best results as compared to open and laparoscopic modalities.
What are the advantages of Robotic surgery?
A Robotic-assisted surgery benefits you directly as well as indirectly. With the advanced camera the surgeon has better visualization, leading to a more precise surgery. Also surgeon has greater range of motion, it’s like having small hands inside the body which can move even 360 degrees and hence one can perform complex dissection and suturing with great ease. Surgeon sees a highly-magnified, high-resolution image of the operating field and has better access to the area being operated on. This leads to fewer complications during surgery, shorter hospital stay, less risk of infection, less blood loss and fewer blood transfusions. Post operatively this leads to less pain, faster recovery and quicker return to daily routine.

Can any Doctor Perform Robotic Surgery?
Without proper training, any doctor cannot simply walk into an operating room and direct a robotic surgery. One has to be certified Robotic surgeon to operate on the system. Not only surgeons, but also entire robotic surgical team has to be specially trained, so that best results are ensured.
What all surgeries are being done with Robotics?
Let us take some examples which were recently done by Dr Rohit Dadhwal and team starting from commonly done to rare ones
35-year-old young female had single episode of left sided pain abdomen on evaluation of which was found to have Left renal mass of size4x3 cm. The patient underwent Robot-aided Partial Nephrectomy on 25th March 2023, wherein only her tumor was removed and rest of the left kidney (almost 80%) was preserved. Histopathological evidence (biopsy report) showed that the tumor had been excised completely. Post operatively, the patient was able to walk on next day of the surgery and discharged on third day and nowhas recovered completely.

77/Male, presented with weak urination and staining while passing urine. His evaluation showed raised PSA and further tests confirmed localised prostate cancer (Stage 1 limited to prostate). Robotic prostate surgery was performed which is considered gold standard in such cases and patient was able to walk the next day. He was discharged and called after 6 weeks for repeat evaluation which showed undetectable PSA and complete cure from tumor.
A young 33 years old male from Kashmir presented with right sided pain abdomen evaluation of which showed large stone which was stuck in ureter (pipe that connects kidney to urinary bladder) with weak kidney. He was told to remove kidney but with the help of Robotic surgery we were able to take out the large stone and save the kidney. With minimal incision he is now completely free of disease and leading a normal healthy life.

A 90 years old man presented with left kidney tumor which was involving whole of the organ. Doing open or laparoscopic was challenging given the age of the patient. He underwent robotic removal of kidney along with tumor which went uneventfully. He was discharged happily on day 3 of surgery. Postoperatively he is now perfectly fine. Not only Robotic surgery is safe and effective it can be offered to patients with any age or comorbidity.

72/Male presented with urine obstruction, Burning urination and Recurrent urinary tract infections. Every time he was given antibiotics and by the time he presented his infection was resistant to all antibiotics. He had undergone multiple surgeries for prostate (at least 6) at various hospitals. On evaluation he was found to have giant UB diverticulum at posterior wall of UB which is abnormal outpouching of bladder. Failure of it to empty led to high residual urine which was the cause of the problem. This was a rare case and Robotic surgery was done for such a big problem. Operation was successful and patient was discharged on second day of surgery.

Another rare case was performed where a young female presented with large mass stuck to urinary bladder neck and urethra (pipe connecting bladder to exterior). Mass was so deep in the abdomen that it was impossible to take it out using traditional open or laparoscopic method. Robotic surgery gave us the chance to remove it completely with ease.
With above examples it is clear that Robotic surgery has become gold standard for not only prostate or kidney tumors but also for rare, tough deep pelvic cases which posed challenge for surgeons for ages. Age has just become a number if we offer robotic surgery
What is the cost of Robotic surgery?
The cost of Robotic Surgery varies based on the type of the surgery being done and the part of the body on which it is being performed. The severity of the case is also a determining factor. It also depends on the the city and the hospital one chooses. The Robotic Surgery price in India ranges from Rs. 1,50,000 to Rs. 4,75,000. Shorter hospital stays and early resumption of duty further decreases financial gap.
What is the future of surgery?
The future of surgery is Robotics and the future of robotic surgery looks promising. Many companies are investing heavily in research and development to improve the technology further. This includes advancements in artificial intelligence, haptic feedback, and increased mobility of robotic arms. With more competition and rise of local players we can expectdecrease the cost of the procedure thereby making it accessible to each and every individual of the society.
Dr Rohit Dadhwal
MBBS, MS (General Surgery) IGMC Shimla
Mch Urology AIIMS New Delhi
Certified Robotic surgeon
Consultant Urology, Andrology and Robotic surgery
Fortis Hospital Mohali
Former Assistant professor Govt Medical College and Hospital Sector 32 Chandigarh
Former Consultant Renal Transplant Fortis Hospital Mohali
This is a well-known fact that Robotic surgery is gold standard for localized prostate cancer and kidney tumors, but what if both the tumors are seen in single patient? In a rare incidence a 70 yr Male, resident of California, USAwith no co-morbidityfound to have increased serum PSA on routine evaluation.USG and mpMRI prostate were suspicious of localized Ca Prostate with left renal mass. CECT KUB done subsequently confirmed left lower polar Kidney mass of size 4.5 x 3 cm which was mostly endophytic reaching till hilum with single renal artery and vein. Prostate biopsy confirmed Adenocarcinoma Gleason score 3+4 and PSMA PET whole body showed localized disease.Hence a diagnosis of Ca Prostate T2NoMo (IG) + left kidney tumor (RCC) T2NoMo (both localized) was made.
Patient came to us with all reports for robotic surgery as he was well aware of the situation that only via robotic modality, he had a chance of being tumor free. We took up the challenge and did Robotic Radical Nephrectomy with Robotic assisted radical prostatectomy with bilateral pelvic lymph node dissection on 28/11/23. Nephrectomy was done first then prostatectomy and total operative time 7 hrs. Both tumors were removed with minimal blood loss <100ml. patient was made ambulatory on POD 1. Drain removed on POD 5 and was discharged on the same day. HPE Prostate- AdenoCaP T2 N0 M0 margin free disease and Kidney- Clear cell RCC margin free. On f/u comfortable, leading a normal life.PSA after 6 weeks 0.01 indicating complete tumor free status.
According to literature 16% of new RCC cases are associated with another malignant tumor and Prostate Ca is the most common concurrent tumor.1 Only 10 cases of roboticradical, or partial nephrectomy (4 + 6) and simultaneous radical prostatectomy have been described.2, 3, 4To our knowledge this is first and only case of simultaneous Robotic radical prostatectomy and radical nephrectomy done in India.
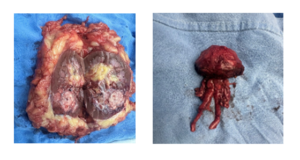
1.Completely endophytic mass left kidney
2.Prostate with seminal vesicles
3. Minimal incision and scarring

1. Beisland C, Talleraas O, Bakke A, Norstein J. Multiple primarymalignancies in patients with renal cell carcinoma: a nationalpopulation-based cohort study. BJU Int, 2006, 97(4):698–702. https://doi.org/10.1111/j.1464-410X.2006.06004.x PMID:16536756.
>2. Lavery HJ, Patel S, Palese M, Kasabian NG, Gainsburg DM, Samadi DB. Combined robotic radical prostatectomy and robotic radical nephrectomy. JSLS. 2010 Oct-Dec;14(4):603-7.
3. Li ZY, Ying CC, Wan ZH, Wang ZS, Li GH, Chen L, Guo YL. Primary prostate cancer synchronous with renal cell carcinoma: clinical experience and literature review. Rom J MorpholEmbryol. 2020 Apr-Jun;61(2):555-561.
4. Cochetti G, Cocca D, Maddonni S, Paladini A, Sarti E, Stivalini D, Mearini E. Combined Robotic Surgery for Double Renal Masses and Prostate Cancer: Myth or Reality? Medicina (Kaunas). 2020 Jun 26;56(6):318. doi: 10.3390/medicina56060318. PMID: 32604918; PMCID: PMC7353895.